“We tell patients it’s going to get harder before it gets easier. We’re not bullshitting anybody,” says Dr Albert ‘Skip’ Rizzo on the phone from his base at the University of Southern California. Rizzo is at the forefront of innovative research into how virtual reality ‘exposure therapy’ – exposing a patient to virtual reconstructions of a traumatic event – can be used to treat patients suffering from post-traumatic stress disorder (PTSD).
The foundations of this work are in the treatment of military veterans, with a ‘Virtual Vietnam’ developed in 1997 to help veterans still suffering with PTSD four decades after the end of the conflict. Virtual reality was first seriously looked at as a tool to treat terror-related PTSD victims four years later, in the month following the September 11 World Trade Center attacks.
The 9/11 firefighter would only move on to more intense reconstructions once a significant reduction in stress was shown
Dr JoAnn Difede from Weill Cornell Medical College and Dr Hunter Hoffman from the University of Washington set out to develop a virtual reconstruction in anticipation of the thousands of disaster workers and civilians who could potentially develop PTSD. A key feature of this first reconstruction was the use of ‘gradual exposure’ – giving a clinician the ability to control the pace of exposure to the virtual world a patient experiences, as well as the nature of the visual and audio stimuli.
The 9/11 reconstruction began with a patient called David, a firefighter suffering from PTSD who had arrived soon after the second plane hit the South Tower. Initially David was exposed to just a virtual reconstruction of a clear sunny day in Manhattan. However, by the third of 10 sessions he began to be exposed to the most intense parts of his experience, like the collapse of the towers.
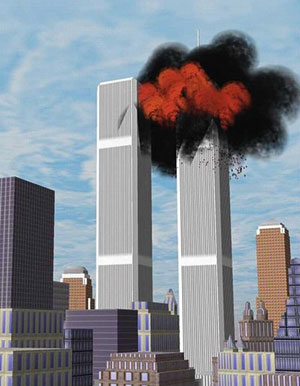
The virtual reality World Trade Center towers are attacked
Key to the treatment was the fact that David would only move on to more intense reconstructions once a significant reduction in stress was shown. With gradual exposure, therefore, patients progress at their own pace.
Difede and Hoffman’s work yielded encouraging results. David reported a 90 per cent reduction in PTSD symptoms, as recorded by the gold-standard Clinician Administered PTSD Scale (CAPS). He experienced a reduction in nightmares and started participating in activities he’d previously avoided due to the trauma. Equally positive results were reported by Difede and Hoffman with a later, slightly larger, 2007 controlled research group.
Advertising helps fund Big Issue’s mission to end poverty
Advertising helps fund Big Issue’s mission to end poverty
Nine out of 10 of the group showed “clinically meaningful” improvements. This was made even more notable by the fact that five of the 10 participants had previously unsuccessfully taken part in other PTSD treatments.
The encouraging results of the original 2002 study led to a growing interest in using virtual reality exposure therapy for treating PTSD in places where attacks were a more common occurrence.
In Israel for instance, a virtual simulation of a suicide bombing at a bus stop called BusWorld was developed. This reconstruction incorporated the same gradual exposure process as the9/11 study, with the first stage ofexposure showing a bus stop with no bus, and the most advanced stage showing the bus on fire after being attacked. This was accompanied with audio recordings of police sirens and even the screams of those injured.
For many people such extreme audio and visual stimuli may seem unnecessary, particularly when compared to more traditional exposure therapy whereby patients recount and describe their traumatic event. Rizzo is aware of such views.
Dr Albert Rizzo puts a patient through the virtual reality experience
He says: “To actually hear the sounds… see the sights of someone screaming or a bomb going off. When I say hard medicine for a hard problem, some people would say torture chamber. Some people say we are going to re-traumatise the person. We haven’t seen this happen.”
For Rizzo it can also be harder to know whether a patient is sufficiently
reimagining the event with traditional therapy. After all, as he says: “You’re asking someone to do exactly what they don’t want to do for months or even years.”
Advertising helps fund Big Issue’s mission to end poverty
Either way, the last few years have seen a greater interest in virtual reality exposure therapy in Europe, with not only rapid technological advancement but also a rise in the number of terror attacks, the latter likely to lead to more PTSD victims. This is because, as a 2015 study by the US Department of Veteran Affairs found, on average 34 per cent of witnesses to bombings and 33 per cent of witnesses to mass shootings will experience a form of PTSD. This is in comparison to only 14 per cent of people who witness a serious road accident.
The November 2015 Paris attacks in particular prompted work to begin on a virtual reconstruction, with a focus on the Bataclan theatre. Virtually reimagining the unimaginable is an expensive business though, and progress stalled due to funding problems. As Rizzo explains: “We started to build the inside of the Bataclan but there’s only so much you can do with graduate students. It does take money to build these things.”
You’re asking someone to do exactly what they don’t want to do for months or even years
This was a problem foreseen by another European academic working on the project, Professor Simon Richir of Institut Arts et Métiers de Laval. Richir explained previously that it was expensive “to reproduce in 3D the places where the attacks occurred and insert avatars of people – dead, alive, injured – and add 3D sound”.
This also requires talented designers, a portion of whom may be reluctant to work on such an emotive project. Creating realistic reconstructions of the events, however, is key to the effectiveness of the treatment. As Rizzo puts it: “You can’t just put out some half-assed development.”
Future technological developments may add even greater realism to the virtual reconstructions, which for now will have an unknown impact on this type of therapy. A fine balance may have to be struck between the benefits of
producing increasingly vivid reconstructions and an even greater focus on not exposing patients to traumatic scenes before they are ready.
Others worry that a future where virtual reality exposure therapy is more common could come at the cost of patients talking and working through their experiences with a clinician. Rizzo stresses though that virtual reality exposure therapy is only one facet of a good overall programme, and a good practitioner is still crucial to any progress. “VR is just a tool to deliver this stuff. You need a good
clinician who knows what they’re doing,” he says.
Advertising helps fund Big Issue’s mission to end poverty
This ‘tool’ continues to be sharpened since its first use on terror-related PTSD following 9/11, in part due to its regular use following combat in Iraq and Afghanistan. VR exposure therapy could potentially help witnesses to the recent mass shooting in Las Vegas.
Closer to home, this form of therapy could help witnesses to major traumatic events such as the Grenfell Tower tragedy and in relation to terrorism. Researchers from the University of Salford are beginning to look at how virtual reality could help witnesses of the Manchester Arena attack earlier this year.
VR is just a tool to deliver this stuff. You need a good clinician who knows what they’re doing
For some people, virtual reality exposure therapy will be seen at best as unnecessary, and at worst as harmful. However, as Rizzo explains: “These are people who don’t understand the science of condition fear and PTSD, they think everything is going to be touchy-feely and nice. I wish it was.”
With terror-related PTSD cases, and PTSD in general unlikely to go away any time soon, this hard medicine could become an increasingly sophisticated and more prominent tool in tackling the hardest of problems.
Advertising helps fund Big Issue’s mission to end poverty